OPINION
New Zealand Doctors Speaking Out with Science
“The most important nairovirus with public-health impact is Crimean-Congo Haemorrhagic Fever virus, which is tick-borne and endemic in much of Asia, Africa, Southern and Eastern Europe.”
International Committee on Taxonomy of Viruses
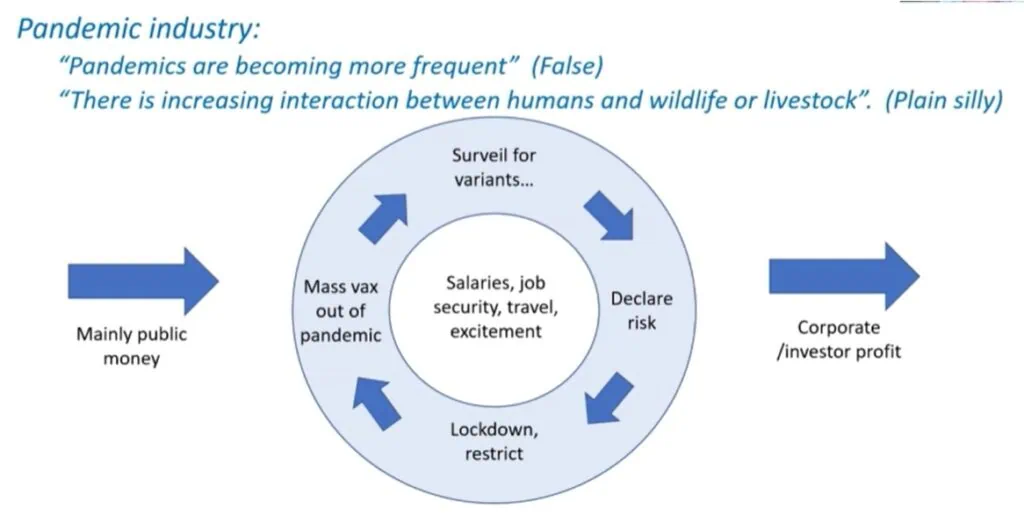
Regular NZDSOS readers will be aware of the obvious plans to introduce more epidemic emergencies as a way to sustain the gold rush brought by covid to those benefiting from the pandemic industry. Marburg Virus, Avian Influenza (“bird flu), Monkey Pox, Swine Flu and frequent simulations practised by those set to gain excessive power and wealth, few of whom have any authentic public health interest or skill, have all featured in recent NZDSOS articles.
Viruses and their naturally-evolving variants are an intrinsic part of environmental and human ecology, both within the human body (our microbiome) and surrounding us in the external environment. The Covid response was a training ground for the limitless possibilities lying in wait as nature is hijacked by a pandemic industry agenda becoming more obvious with each passing day.
Keeping up with the next “disease rollout” is no mean feat as multiple diseases of concern appear in frightful headlines on what seems like a daily basis. Since at least as early as March last year, Crimean-Congo Haemorrhagic Fever has headlined irregularly, and it is making more frequent appearances in mainstream media at the moment. Investigative journalist Jefferey Jaxen discussed the issue of ongoing media-driven fearmongering and the historical connection with biological laboratory research in relation to Crimean-Congo Haemorrhagic Fever on The Highwire this week.

First Principles of Infectious Disease Diagnosis
Every infectious agent (each species of virus, bacteria, fungus and parasite) has it’s own individual ways to breach the defences of the human body. For example SARS-CoV-2, the virus responsible for Covid, is inhaled and must then bypass various defences in the respiratory tract before it can cause disease; whereas the nairovirus responsible for Crimean-Congo Haemorrhagic Fever can only cause disease via direct entry into the bloodstream (usually via the bite of an infected tick).
Similarly, every human body has uniquely different defence mechanisms depending on factors such as age, nutritional status, prior exposure and immune function. Regardless of the infectious agent, disease can only establish when each of the following steps occur.
- Encounter: the agent (virus) meets a host (human);
- Entry: the virus enters the human body;
- Spread: the virus spreads from the entry site towards specific cells (different for each virus);
- Multiplication: viruses can only multiply inside cells of individuals they infect (which specific cells depends on the virus species);
- Damage: the virus, and/or the immune reaction to the virus, cause tissue damage;
- Outcome: ranges from death, permanent damage or temporary illness, to the virus exiting the body, or the virus persisting within the body without causing damage.
As such, the mere presence of an infectious organism is not enough to make a disease diagnosis, which requires tissue damage leading to illness. This basic principle was turned on its head during the covid pandemic, with the use of both Polymerase Chain Reaction (PCR) and Rapid Antigen Testing (RAT). Both of these tests may determine (sometimes erroneously), the presence of virus particles in a sample of body fluid/tissue. The tests do not inform us beyond Step 2 (entry), thus telling us nothing about the presence or absence of disease. With only one organism tested for, they also ignore the range of other possible causes when disease is present.
Once tests such as PCR and RAT were a small component within a complex clinical investigation undertaken by medically trained personnel. Their incorrect use has removed clinical skill from the diagnostic process. For now, this is a problem specific to covid, although influenza has been added to some RAT home kits. However, the destruction of skilled medical diagnosis seems inevitable until doctors stop complying with the demise of their own profession.
Crimean-Congo Haemorrhagic Fever Virus
Crimean-Congo Haemorrhagic Fever virus is one of many RNA viruses from distinct virus families, which can cause viral haemorrhagic fever (VHF). Other well-known VHF diseases include Dengue and Yellow Fever (Flavivirus family), Marburg and Ebola (Filovirus family) and Rift Valley Fever (Phenuivirus family). There are many other lesser-known viral haemorrhagic fevers, all of which can cause similar or identical disease, but which do not necessarily share genetic traits.
According to the International Committee on Taxonomy of Viruses there are 14 species within the Orthonairovirus genus, four of which may infect humans. Crimean-Congo Haemorrhagic Fever Virus is the only one which causes severe (VHF) disease in humans. It is endemic throughout areas inhabited by the Hyalomma tick, being South-East Asia, the Middle East, Africa and parts of Europe.
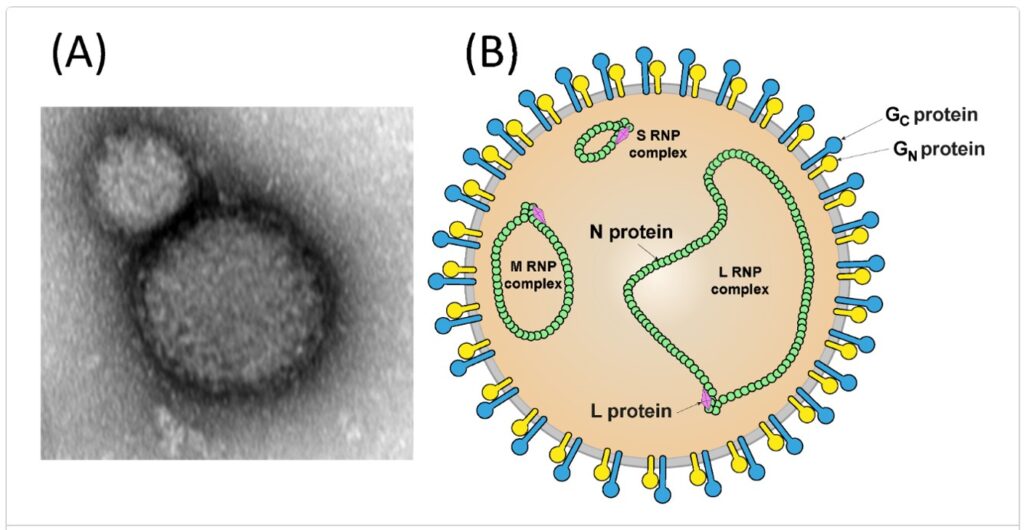
Most Orthonairoviruses are transmitted by ticks, which act as an intermediary between infected animals and uninfected animals. The virions (single virus) are round with glycoprotein spikes on their surface, and their genetic material consists of three circular, single strands of RNA.
(A) is an electron micrograph of a Crimean-Congo Haemorrhagic Fever virus.
(B) is a schematic illustration of a nairovirus particle and it’s most important components (proteins and genetic material).
Crimean-Congo Haemorrhagic Fever Disease
According to the World Health Organization, the disease was first described in 1944 in the Crimean Peninsula (now part of Ukraine). Initially named Crimean Haemorrhagic Fever, in 1956 an identical illness was identified in the Congo Basin (central Africa), which was subsequently recognised as being caused by the same virus, hence the updated name.
Crimean-Congo Haemorrhagic Fever is transmitted via the bite of a specific type of tick (Hyalomma species), although other species may also play a role in transmission. Very rarely, the virus may enter the bloodstream directly via exposure to the blood of an infected animal through a break in the skin.
Although case fatality rates are reported at between 10-40% it is important to remember that this represents the fatality rate of those people who present to health facilities in need of care. Seroprevalence studies (eg Iran in 2012, Greece in 2013 and Nigeria in 2016) show that the virus is endemic in regions where the Hyalomma tick is found, particularly among populations in close contact with livestock, suggesting that exposure leads to high rates of asymptomatic infection (as outlined above, this does not meet the criteria for disease), or mild disease.
In symptomatic disease, the incubation period of Crimean-Congo Haemorrhagic Fever is commonly 1-3 days but may take as long as 9 days. Many symptoms are non-specific, such as headache, malaise, fever and muscle aches. Where damage occurs to the lining of the blood vessels, low blood pressure, multiple organ failure and shock can be lethal. Destruction of blood cells can occur, including platelets which can lead to excessive bleeding, hence the name for this severe form of the disease: ‘viral haemorrhagic fever’.
Patient treatment can include antiviral therapies (ribavirin) if given early enough in the progression of disease. Otherwise supportive therapy to manage symptoms is recommended. The best prevention is common sense approaches such as avoiding tick bites, covering breaks in the skin and hand hygiene after touching animals.
Why is Crimean-Congo Haemorrhagic Fever Making Headlines?
Today’s legacy media are irresponsibly referring to Crimean-Congo Haemorrhagic Fever as “Killer Virus”. Whilst, as with all viruses, it has a potential to be lethal, it is clear that most people exposed to the virus will experience asymptomatic or mild infection, or moderate to severe infection followed by a full recovery, particularly when appropriate medical care is provided.
The USA Undersecretary of State for Political Affairs, Victoria Nuland has confirmed that biological research facilities are located in the Ukraine. Russian President Putin has accused the Pentagon of carrying out a biological weapons program in the Ukraine, on the Russian border. The research includes Crimean-Congo Haemorrhagic Fever studies financed and conducted by American biologists.
There are reports of an unmanageable increase of infections being seen in the Ukrainian health system including Tuberculosis and Measles. An emergency phasing out of the programs is reportedly underway with plans to continue the military program outside of the Ukraine.
Human rights lawyer and leading expert in biological law, Dr Francis Boyle has implicated Australia’s Doherty Institute in this bioweapons program. The Doherty Institute was largely responsible for the mathematical modelling which claimed justification for Australia remaining locked down until high rates of vaccination were achieved. Russia has accused those involved in these research facilities of “carrying out work to enhance the pathogenic properties of microorganisms…” Learn more here and here.
Climate change is being blamed for the alleged spread of Crimean-Congo Haemorrhagic Fever. This is highly coincidental and convenient given the plans for the World Health Organization One Health policy to include strict control of human behaviours to reduce the impact of climate change as well as human-animal-plant-ecosystem interactions. The infographics being used seem to support the idea that WHO plan to take charge of all global systems under the One Health banner.
Meanwhile, eminent scientists dissenting from the climate change narrative have experienced the same levels of censorship more recently faced by countless medical doctors and scientists. Learn more from Greenpeace founder Dr Patrick Moore; geologist Gregory Wrightstone; and Nobel Prize-winning physicist Dr John Clauser.
One final piece of the jigsaw puzzle is, of course, the plan for further vaccination revenue. In their “Global Public Health Strategy”, Moderna – who had never brought a product to market until 2020 – announced “15 vaccine programs targeting emerging or neglected infectious diseases by 2025“, of which Crimean-Congo Haemorrhagic Fever is one.
Conclusion
The gold rush that was Covid has created a murmuration of converging opportunists, some of whom are extremely powerful and some undeniably carrying out criminal acts. The majority of opportunists, however, are those who would argue that they are “just doing their job“. Health professionals complying with useless and harmful medical interventions whose only purpose is to commercialise “health care”; media pundits unquestioningly promoting the narratives serving their powerful paymasters; politicians toeing the party line rather than speaking out on behalf of the people they purport to represent.
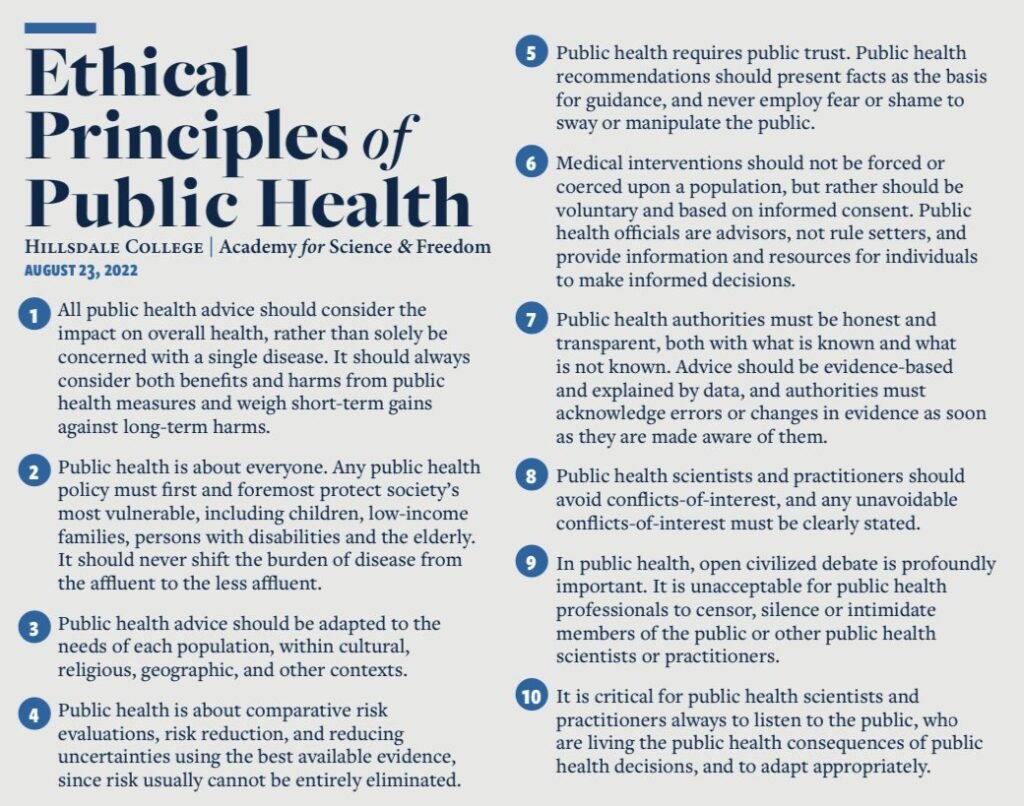
We once more ask our medical and allied health colleagues to look at the ethical principles of public health, including the importance of optimising health before stepping up to the more expensive options, and defend them. Join NZDSOS in the fight against criminalised, cookie-cutter, profit-driven medicine, for a return to authentic, beneficial health care that aims to promote health and prevent disease.