


Ramesh Thakur
brownstone.org
Ramesh Thakur, a former United Nations Assistant Secretary-General, is emeritus professor in the Crawford School of Public Policy, The Australian National University.
Deborah Birx was the White House Covid-19 response coordinator under President Donald Trump. Jeffrey Tucker recently wrote a brutal takedown of her deliberate misrepresentations of science and data in order to manipulate Trump into going along with her preferred but misguided policy interventions to deal with the Covid outbreak.
In an ABC podcast on December 15, 2020, she said: “I understand the safety of the vaccine … I understand the depth of the efficacy of this vaccine. This is one of the most highly-effective vaccines we have in our infectious disease arsenal.”
Appearing on Fox News on July 22, however, she claimed: “I knew these vaccines were not going to protect against infection. And I think we overplayed the vaccines. And it made people then worry that it’s not going to protect against severe disease and hospitalization.”
This might help to explain why there has been such a concerning collapse of public confidence in leading health institutions and “authorities”.
Biden’s claim of a pandemic of the unvaccinated
During a CNN Town Hall event on July 21, 2021, President Joe Biden said: “If you’re vaccinated, you’re not going to be hospitalized, you’re not going to be in an ICU unit and you are not going to die.”
On May 16, 2021, Dr Anthony Fauci claimed that vaccination did not just protect the individual, but also the community, because “by preventing the spread of the virus … you become a dead end to the virus. And when there are a lot of dead ends around, the virus is not going to go anywhere.”
Relying in the judgment of his chief medical adviser, Biden took to talking about the pandemic of the unvaccinated in a two-track effort both to encourage vaccine take-up and to vilify, demonize and shame those who remained uncertain enough of the balance of benefits and short and long-term risks of the rushed Covid-19 vaccines to avoid succumbing to the multiple pressures to go along with the zeitgeist in order to get along with everyone.
We have now had both Dr Fauci, the public face of the US management of the pandemic, revered in some quarters and reviled in others, and President Biden himself get infected with Covid, despite both being double-vaccinated and double-boosted.
Inevitably, to try and stop the official narrative on the benefits of the vaccine from unraveling completely and in order to encourage continuing vaccine and boosters take-up, they insist that their updated vaccination status helped to limit the severity of their infection. This is based on a cult-like faith, akin to self-validating and self-canceling explanations put forth by astrologers for predictions that come true and don’t, as the case may be.
Although on July 20, Fauci admitted that the data do make it clear that “vaccines – because of the high degree of transmissibility of this virus – don’t protect overly well, as it were, against infection.” Robert F Kennedy Jr asked why the media was not holding Fauci “accountable for the costly national policies and the lockdowns that were utterly built upon his initial assertion that the vaccines would prevent transmission and end the pandemic.”
Equally, of course, one must ask again: if vaccines don’t stop transmission, how does the government justify vaccination mandates for travel to the US?
In a matching vein, the New South Wales (NSW) health report for the week ending 16 July claims that: “The minority of the overall population who have not been vaccinated are significantly overrepresented among patients in hospitals and ICUs with Covid-19.”
The following challenges that claim using their own data.
By drawing on the distinction between the efficacy and effectiveness of vaccines, it’s possible to argue that in NSW, rather than a pandemic of the unvaccinated, what we have witnessed is a pandemic of the triple-vaccinated.
NSW health facts
In September 2021, NSW had 844 staffed ICU beds, of which 173 (20.5 per cent) were occupied by Covid-19 patients. (Australia-wide, the number of ICU beds is 2,183.) By January 2022, the number had increased to around 1,000. If necessary, this can be bumped up further by utilizing the limited number of ICU beds in private hospitals.
There are 9,500 general ward beds in public and another 3,000 beds in private hospitals in NSW. In mid-July 2022, there were 2,058 people in hospital with Covid-19 in NSW, or 21.7 per cent of the public system’s capacity and 16.5 per cent of the state’s total hospital beds capacity. An additional 6,500 people were in hospital for non-Covid reasons.
During the week of July 10-16, a total of 806 people were admitted to hospital with Covid-19, another 77 into ICU, and 142 people died with Covid-19 illness (though not necessarily as the primary cause of death). Moreover, of the 142 deaths, only four were aged below 60, so that people aged 60 and above accounted for 97.2 per cent of all Covid-related deaths in the state.
Additionally, of the 142 dead, the vaccination status of two was not known. One hundred and eighteen of the remaining 140 – 84.3 per cent – were at least double-vaccinated and 69 had received three doses of the vaccine: by far the biggest single cohort and almost equal to all the others combined. Hence the thought that perhaps what we are experiencing is a pandemic of the triple-vaccinated.
Efficacy vs effectiveness
The Cambridge Dictionary defines efficacy as “how well a particular treatment or drug works under carefully controlled scientific testing conditions”. By contrast, effectiveness is defined as “how well a particular treatment or drug works when people are using it, as opposed to how well it works under carefully controlled scientific testing conditions”.
Thus doubts about the effectiveness of a new product in treating any disease can only be resolved once the vaccine is widely available and administered in the target population. GAVI (the Global Alliance for Vaccines and Immunization), now called Gavi, the Vaccine Alliance, is a partnership between the World Health Organization, Unicef, the World Bank and the Bill & Melinda Gates Foundation.
Writing for GAVI, Priya Joi offers similar definitions, describing “efficacy” as the measure of how much a vaccine prevents infection (and possibly also transmission) under ideal, controlled conditions where a vaccinated group is compared with a placebo group. She adds: “Vaccines do not always need to have an exceptionally high effectiveness to be useful, for example the influenza vaccine is 40-60 per cent effective yet saves thousands of lives every year.”
Examining the percentage of the thrice-jabbed in hospital admissions, ICU beds and dead against the baseline of their share in the overall population, preferably age-adjusted, is critical to calculating vaccine efficacy. I’m not sure how helpful that is to assessing the effectiveness of vaccines in keeping the absolute numbers down below the state’s or country’s capacity thresholds of hospital and ICU beds.
If the primary public health justification for universal vaccination is to reduce the burden on the health infrastructure and prevent hospitals and ICU capacity from being overwhelmed – which was indeed the main justification in the language of two-three weeks to flatten the curve – then the key question becomes: How effective are the vaccines in preventing hospital admissions and ICU occupancy? Their role in preventing infection by itself is less important than their effectiveness in controlling the severity of the disease.
For example, a report from the Dutch health ministry found that the effectiveness of two doses of vaccines after one year had fallen overall to zero per cent against hospitalizations and minus 20 per cent against ICU admission. Perhaps more pertinently in relation to NSW, Dr Eyal Shahar notes signs in Israel of a short-term fatality rate of a third dose.
Efficacy is more helpful to an individual in assessing the relative risk of infection if vaccinated or not. Because Covid vaccines were granted emergency-use authorization and long-term efficacy and safety profiles were simply not available, doubts have persisted about the integrity, credibility and long-term reliability of data and results from the trials conducted by the vaccine manufacturers.
Moreover, as we’ve been made aware with respect to the UK, different branches of the government like the Health Security Agency and the Office of National Statistics use different and hotly contested methodologies for calculating the numbers and proportions of the population infected by Covid, which in turn determines the estimated infection fatality rate (IFR).
In any case, even if we agree that the IFR and case fatality rate (CFR) of flu and Covid are broadly comparable by now, the scale and magnitude of Covid means that similar IFR and CFR still produce vastly different orders of challenges for public health policy.
By contrast the effectiveness of the vaccines for controlling hospital admissions, ICU bed occupancy and mortality is measured by solid and reliable information that is both accurate and comprehensive in Western countries. This makes vaccine effectiveness a better policy tool for deciding on population-wide mandates, while efficacy might be the more relevant for informed individual decisions.
Covid in NSW
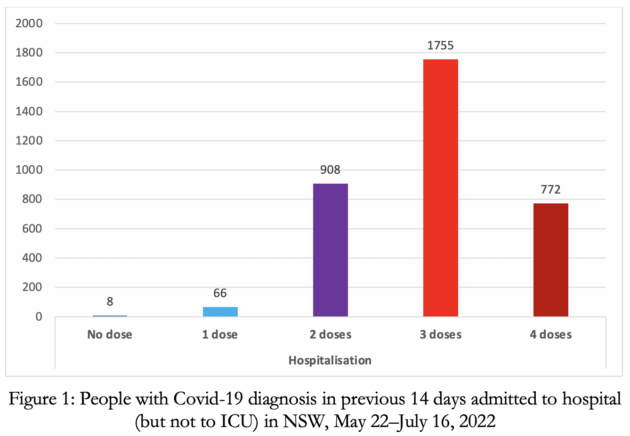
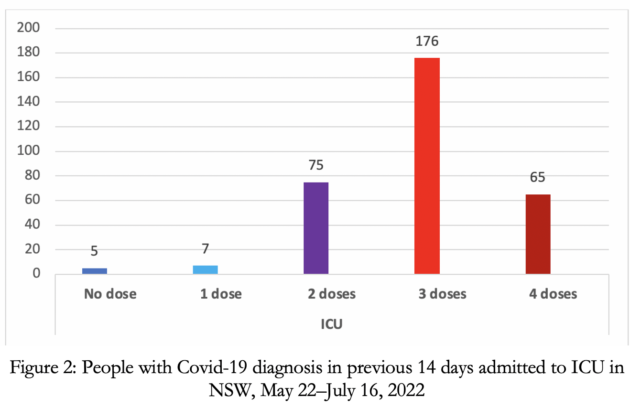
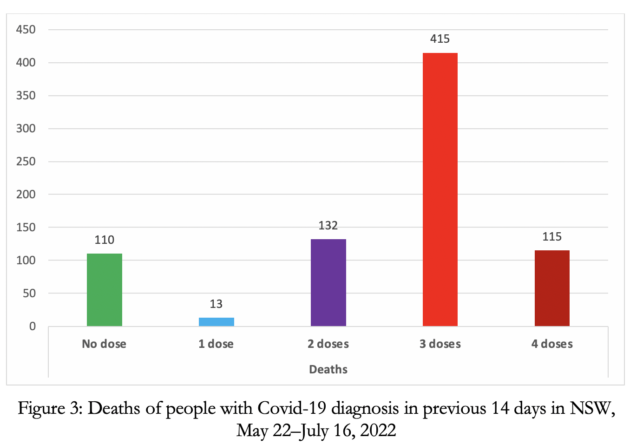
In the period for the weeks ending May 28 to July 16, 2022 in NSW, of those whose vaccination status was known, only eight unvaccinated people were among the 3,509 who required hospital admission (Figure 1). The numbers in ICU were five unvaccinated and 316 with two to four doses (Figure 2); the number of Covid dead were 110 unvaccinated and 662 with two to four doses (Figure 3).
With 83 per cent of people at least double-vaccinated, they accounted for 99.4, 96.3 and 85.4 per cent, respectively, of NSW Covid hospital admission, ICU and deaths in these seven weeks.
In the final week of this seven-week period, of those whose vaccination status was known, there were exactly zero – zilch, nada – unvaccinated people among the 624 hospital and 59 ICU Covid-19 admissions, compared to 615 with two, three and four vaccine doses in hospital and 58 in ICU beds. Just the triple-vaccinated, who account for 68 per cent of the population of NSW, made up 57.5 per cent in hospital, 53.7 per cent in ICU and 53.5 per cent of the Covid dead.
The claim that the unvaccinated are “significantly overrepresented” in Covid-19 hospital admissions and ICU occupancy is not just misleading, it’s downright false. Seriously, do they look at the data in their own reports before drawing policy conclusions?
As knowledge about the rapidly fading efficacy of the vaccines, and in particular of each successor booster dose, has firmed, and also as the vaccine escape properties of the newer variants of Covid-19 have become better known, the equivalent question now is: are we into the era of the pandemic of the triple-vaccinated? The biggest strain on NSW hospitals and ICU beds is coming from their numbers.
Public health officials can talk and dissemble all they want about the baselines for comparisons and pretend to possess great sophistication in their understanding of the current state of the disease. They still cannot spin their way out of the hard data.
Instead they are exhibiting a severe case of cognitive dissonance in encouraging the double-vaccinated to get boosted and double-boosted. The ineffectiveness of vaccines in reducing hospital admissions and ICU demand is in itself sufficient to torpedo vaccine mandates. Doubts on their efficacy and concerns about their adverse effects and long-term safety further strengthens the case against mandates.