


Eyal Shahar
brownstone.org
Dr. Eyal Shahar is a professor emeritus of public health in epidemiology and biostatistics. His research focuses on epidemiology and methodology. In recent years, Dr. Shahar has also made significant contributions to research methodology, especially in the domain of causal diagrams and biases.
Dogmatically adhering to slogans, regulators have not tried to estimate the rate of fatal consequences of Covid vaccines. We are left to search for estimates using indirect methods.
The circumstances around the third-dose (“booster”) campaign in Israel provide unique insight into a possible range of the short-term fatality rate. Long-term, vaccine-related mortality will be more difficult to quantify.
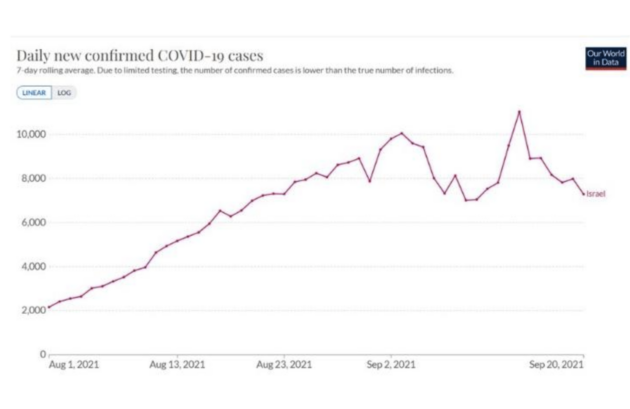
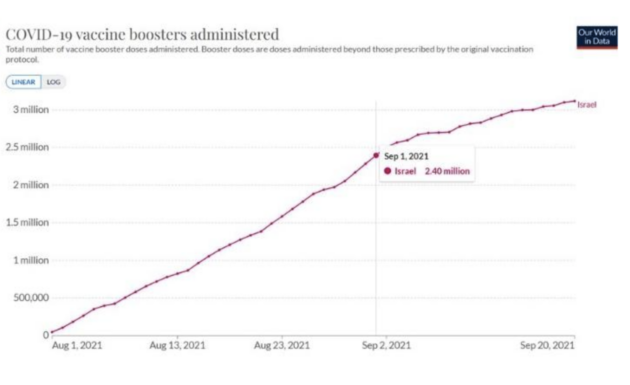
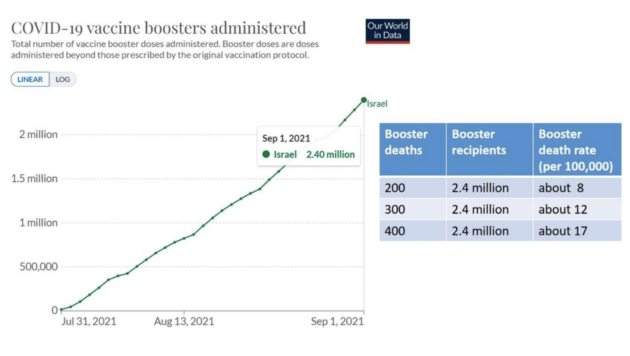
At the end of July 2021, the ministry of health approved the booster for those who were at least 60 years old, and about 2.4 million residents were vaccinated in August – during the rise of a Covid summer wave.
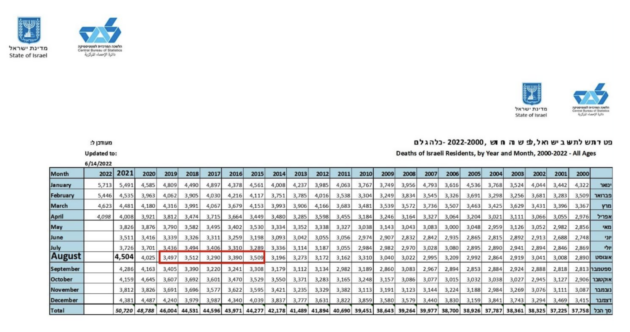
The Israel Central Bureau of Statistics counted 4,504 deaths, from all-causes, during the month of August 2021. How many were expected? How many fall in the category of excess deaths?
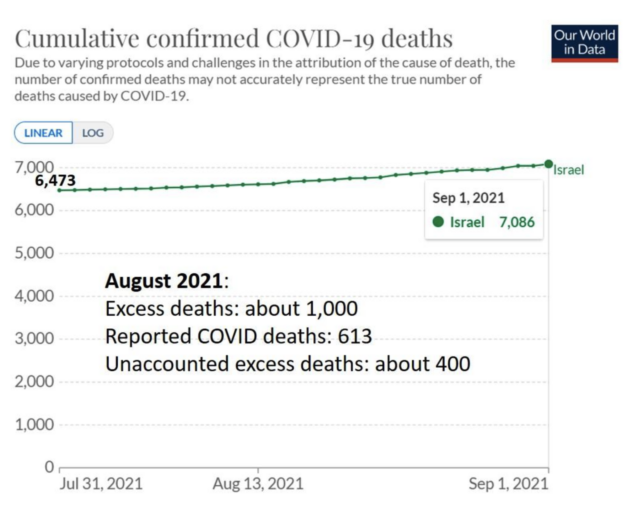
Importantly, the “normal” number of deaths in August has been fairly stable just before the pandemic, capped at about 3,500 between 2015 and 2019 (red rectangle). Using that baseline, the excess mortality of about 500 in August 2020 is compatible with Covid and panic-related deaths. The estimated number of excess deaths in August 2021 is twice as high: about 1,000.
How many Covid deaths were reported in August 2021?
613
This implies about 400 unaccounted excess deaths. Are these booster-associated deaths?
So far the data seem straightforward, but there are several sources of uncertainty about the split of excess deaths between Covid deaths and unaccounted deaths in August 2021:
- Booster recipients were less likely to be diagnosed as cases (and therefore to be called Covid deaths, if they died) because people might have attributed their Covid symptoms to the booster and did not get tested. Likewise, there was a general tendency to not test booster recipients as rigorously as others. Therefore, the number of true Covid deaths among booster recipients should be larger, and the number of unaccounted deaths – smaller.
- On the other hand, there was a tendency in Israel (and elsewhere) to over-count Covid deaths – sometimes substantially. During the previous winter (December 2020 through March 2021), the estimated number of excess deaths was half the number of reported Covid deaths, which means that half of reported Covid deaths were “death with Covid,” not “from Covid.” If that level of misclassification persisted in August, the number of true Covid deaths should be smaller, and the number of unaccounted excess deaths – much larger.
- The early post-vaccination period is a high-risk period – for contracting Covid and for death from Covid. Since the ministry of health decided to administer the booster concurrent to a rising wave, some Covid deaths might have been caused by the booster/im
- Some unaccounted deaths might have been the result of avoiding or delaying urgent medical care for non-Covid conditions, the consequences of panic.
There is no way to quantify the net effect of these mechanisms, but a conservative approach (favouring the booster) might put the upper limit of booster deaths at 400 and reduce that number to 300 and 200. A plausible range of the booster fatality rate in Israel in August 2021 is shown in the table: 8 to 17 deaths per 100,000 vaccinees.
In a recent article, Gibson studied the association between the booster rollout in New Zealand and rising excess mortality. He estimated 16 excess deaths per 100,000 booster doses (95% CI: 5 to 27). The results from Israel fall in that range.
A vaccine with a mortality rate on such a scale is not “safe” – at least according to public health standards that had been applied to the flu vaccine and other vaccines. Nor is it “safe” according to estimates of serious adverse events from randomized trials.
At a minimum, the estimated fatality rate should be part of informed consent. Unfortunately, informed consent has not been on the agenda of officials since Covid vaccines entered the market through emergency use authorization.